The Main Types of Skin Cancer
Melanoma
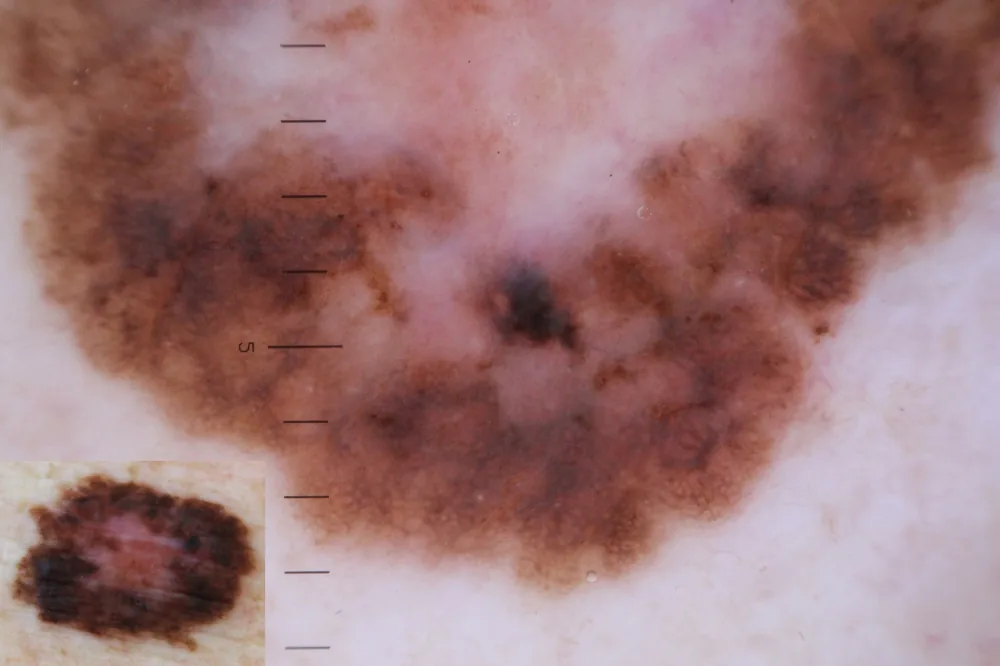
Melanoma originates from melanocytes, the cells that produce melanin. It is the most aggressive skin cancer because it can metastasise if not diagnosed early. Its prognosis depends heavily on the stage at diagnosis: in in-situ and stage I forms, 5-year survival rates are very high (in many series above 90%); in more advanced stages the prognosis becomes progressively less favourable. Melanoma can develop from pre-existing moles or, more frequently, on apparently healthy skin. The ABCDE rule is a useful tool for recognising lesions that warrant specialist attention.
Basal Cell Carcinoma (BCC)
Basal cell carcinoma is by far the most common skin cancer. It grows slowly and is locally invasive, but it rarely metastasises. It is strongly correlated with chronic sun exposure and is typically located in sun-exposed areas: face, nose, ears, scalp. The prognosis with prompt treatment is excellent.
Squamous Cell Carcinoma (SCC)
Squamous cell carcinoma is the second most frequent skin cancer. It can develop from pre-existing actinic keratoses, has metastatic potential in certain sites and clinical situations, and is associated with cumulative sun damage. It generally requires surgical removal with margin control, performed on an outpatient basis or — in more complex cases — in a hospital setting.
Precancerous Lesions
Actinic keratoses are precancerous lesions caused by chronic sun damage, with the potential to evolve towards squamous cell carcinoma. They appear as rough, scaly patches on sun-exposed areas. They can be treated with non-invasive therapies — including photodynamic therapy — and treating them reduces the risk of progression to cancer.
The ABCDE Rule for Recognising Suspicious Moles
The ABCDE rule is a self-examination tool useful for recognising pigmented lesions that require a specialist assessment.
- A — Asymmetry: a normal mole is generally symmetrical; if divided in half, the two parts should be the same
- B — Irregular borders: jagged, notched or poorly defined borders can be a warning sign
- C — Uneven colour: variations in colour within the same mole (light/dark brown, black, bluish, reddish, white)
- D — Diameter greater than 6 mm: moles larger than a pencil eraser deserve attention
- E — Evolution over time: changes in size, shape, colour, thickness or consistency
Other signs not to underestimate: spontaneous bleeding, persistent itching, the formation of crusts that do not heal, rapid growth, the appearance of nodules. Periodic self-examination is important, but it does not replace a specialist check-up.
Our Specialist Experience
Diagnosis with VIDIX Dermoscopy
The accurate diagnosis of skin cancers requires specific expertise and adequate instruments. We use the VIDIX digital dermatoscope for the microscopic analysis of skin lesions. Dermoscopy makes it possible to assess structures and features that are not visible to the naked eye, significantly increasing diagnostic accuracy and reducing the number of unnecessary biopsies.
Systematic Approach
- ✓ Complete personal and family history
- ✓ Full clinical skin examination, including scalp, palms, soles, genital region and mucous membranes
- ✓ Digital dermoscopy of clinically relevant lesions
- ✓ Photographic documentation for follow-up
- ✓ Risk classification according to international guidelines
Biopsy and Histological Examination
When a lesion is clinically suspicious, the definitive diagnosis requires a skin biopsy with histological examination. For small lesions, an excisional biopsy may be indicated, which allows diagnosis and treatment in a single outpatient procedure.
Treatment Pathway
Once the histological diagnosis has been obtained, Centro Eudermia defines the most appropriate pathway: for benign or low-risk lesions, removal is performed on an outpatient basis at the practice. For melanoma and skin cancers with a more severe prognosis, Centro Eudermia refers the patient to the hospital oncology pathway for oncological surgery with adequate margins and multidisciplinary management. Long-term dermatological follow-up remains at the centre for the prevention of recurrences and the monitoring of the risk of new lesions.
Risk Factors: Who Should Have Screening
High Risk (every 6-12 months)
- • Very fair skin, light-coloured eyes
- • Numerous moles (more than 50)
- • Personal/family history of melanoma
- • Severe sunburn in childhood
- • Use of tanning beds
- • Prolonged outdoor work/sport
- • Immunosuppression
Moderate Risk (annually)
- • Fair skin, tendency to burn
- • 20-50 visible moles
- • Occasional intense sun exposure
- • Age over 40
- • History of non-melanoma skin cancers
Low Risk (every 2 years)
- • Dark skin that tans easily
- • Few moles (fewer than 20)
- • No family history
- • Consistent sun protection
Prevention
Prevention is the first tool against skin cancer. The main recommendations include:
- ✓ SPF 50+ sun protection daily, even on cloudy days
- ✓ Reapplication every 2 hours during exposure
- ✓ Avoid direct exposure in the middle of the day (11 am to 4 pm)
- ✓ Protective clothing, a wide-brimmed hat, sunglasses
- ✓ Never use tanning beds (classified as group 1 carcinogens by the WHO)
- ✓ Education in sun protection from childhood
- ✓ Periodic self-examination of the skin
- ✓ Mole mapping for those with risk factors
Frequently Asked Questions About Skin Cancer
Early diagnosis is essential in skin cancer. The information on this page is for general information and educational purposes only and does not replace a specialist medical assessment. The prognosis of skin cancers depends on numerous factors and should always be discussed with your own specialist.